Welcome to My New Mental Health Blog
I didn’t know much about adolescent mental disorders until we had to read John Breeding’s entitled, Electroshocking Children: Why It Should Be Stopped. I wasn’t even aware that this was something that was happening, let alone that it should be stopped.
Before I decided to dive deeper into unjust adolescent treatments on children that are mentally ill, I wanted to learn more on the history of adolescent mental issues treatment.
THE START
1899
Before people believed the idea of children having mental disorders, pediatric psychiatric disorders were ignored or blamed on poor upbringing. It wasn’t until 1899, that the nation’s first juvenile court was established in Chicago, Illinois. This occurrence led to the board of directors of Jane Addam’s Hull House to see a look into juvenile delinquency. They wanted to understand its origin, prevention and treatment.
Early 1900s
In 1909, these women created the Juvenile Psychopathic Institute. It was during this time that they hired a neurologist named, William Healy, M.D., to be the institute’s first director. He began studying the children’s brain functioning, IQ, social factors, attitudes and motivations. To accomplish these broad evaluations and treatment strategies, Healy formed teams composed of a neuropsychiatrist, a psychologist and a social worker. This approach became the template used today by most child guidance clinics for most of the 20th century.
Late 1900s

With the rise of pediatric psychiatric disorder awareness, came more and more people trying to cure it, including the controversial Lauretta Bender. Bender was one of the first American physicians to treat and study children with schizophrenia and severe emotional disturbance, however, her educational background had not prepared her to work for children because child psychiatry training didn’t exist at the time.
One positive thing about Dr. Bender is that she wasn’t judgmental toward the parents of the patients she saw. She encouraged sympathy for parents who faced the challenge of caring for children she labeled as, “unresponsive, unpredictable offspring.” However, Dr. Bender began administrating Electroconvulsive therapy (ECT), major tranquilizers like Thorazine, hallucinogens like Lysergic Acid Diethylamide (LSD), and other psychoactive drugs to children as young as three years of age.
What is Electroconvulsive Therapy?
Electroconvulsive therapy, or ECT, involves the mass production and delivery of a grand mal convulsions to the brain. It is a scientifically epileptic seizure that manually passes 600 volts of electric currents through the brain for up to four seconds, creating convulsions that lasts up to 60 seconds. Before the traumatic experience, patients were given anesthetics and drugs to paralyze the muscles, to suppress fear and pain, and to minimize the number of broken bones. Doctors found before the use of anesthetics and drugs, patients often suffered broken bones, including bones in their spines.
Results of Electroconvulsive Therapy
The effects of Electroconvulsive Therapy may produce life-threatening complications, such as apnea, cardiac arrest, and even death. After the convulsions caused by the Electroconvulsive Therapy, patients often experience several minutes of unconsciousness. Electroshock is usually administered in hospitals equipped to handle emergency situations, including death, that may develop during or soon after the shock.
The Fight Against It
Many people have always been against Electroconvulsive Therapy. In 2001 during a hearing against Electroconvulsive Therapy before the New York Assembly Standing Committee on Mental Health, Mental Retardation, and Developmental Disabilities, neuroscientist Dr. Peter Sterling (pictured above) argued the following:
“ 1) ECS is designed to evoke a grand mal epileptic seizure involving massive excitation of cortical neurons that also deliver excitation to lower brain structures. The seizure causes an acute rise in blood pressure well into the hypertensive range, and this frequently causes small hemorrhages in the brain. Wherever a hemorrhage occurs in the brain, nerve cells die — and nerve cells are not replaced.
2) ECS ruptures the ‘blood-brain barrier.’ This barrier normally prevents many substances in the blood from reaching the brain. This protects the brain, which is our most chemically sensitive organ, from a variety of potential insults [injuries]. Where this barrier is breached, nerve cells are exposed to insult and may also die. Rupture of this barrier also leads to brain ‘edema’ (swelling), which, since the brain is enclosed by the rigid skull, leads to local arrest of blood supply, anoxia [lack of oxygen], and neuron death.
3) ECS causes neurons to release large quantities of the neurotransmitter, glutamate. This chemical excites further neuronal activity which releases more glutamate, leading to ‘excito-toxicity’ — neurons literally die due to overactivity. Such excito-toxicity has been recognized relatively recently and is now a major topic of research. It is known to accompany seizures and over repeated episodes of ECS may be a significant contributor to accumulated brain damage.” [2]
TODAY
Electroconvulsive Therapy or Drug Use?
While many psychiatric professionals are stepping away from Electroconvulsive Therapy, many are now turning to prescription drug use. The National Survey of Children’s Health conducted an analysis of health data where they found that one in six children of the United States between the ages of 6 and 17 have a treatable mental health disorder. These disorders are commonly diagnosed as depression, anxiety problems or attention-deficit/hyperactivity disorders. this analysis also found that almost half of these children with at least one of these disorders, have not received treatment or counseling from a mental health professional. [3]
Through my research, I found that similar to the novels that we have read in class and much like Dr. Bender, physicians are more likely to turn to drugs to treat these children.
According to Jeannette Y. Wick, the assistant director of the Office of Pharmacy Professional Development at the University of Connecticut School of Pharmacy in Storrs, in the past decade, physicians have been more likely to prescribe antipsychotic medications to children, than ever before. Her research found that more than 1 million American youths take antipsychotic drugs, and that antipsychotic prescribing for adolescents in the United States increased by 50%. The image below depicts a table of the FDA approved drugs that are given to children, with their diagnoses, and ages.
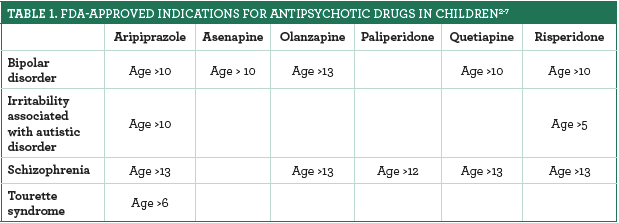
When I dug deeper into the antipsychotics given to children as young as 5 years old, I found that it is not a surprise that these drugs can cause the following side effects: muscle rigidity, slow movement, involuntary tremors, substantial weight gain, an increased risk of type 2 diabetes, and elevated cholesterol levels. These risks are too dangerous for young children such as 5 and 6 years old. These children aren’t clearly able to express themselves well, so turning to drugs at such a young age, shouldn’t be a huge option.
If parents are not careful with their selection of treatments, these drugs can prevent lifelong and serious complications. Upon further research, I found that antipsychotic medications are approved only for treatment of bipolar disorder in children between the ages of 10-17 and for schizophrenia in children between the ages of 13-17. They are also approved to treat the irritability that accompanies autism and effects of Tourette syndrome. This means that many of these prescription drugs that are being given to children are considered “off-label” because they are not approved by the FDA. The FDA has not approved pediatric use of many of these drugs because there is not enough scientific evidence to support it. This leads me to believe that without proper examination, many children are being improperly diagnosed and treated incorrectly, the same way Dr. Lauretta Bender believed she was treating those children correctly.
[1] -Schowalter, John E. “A History of Child and Adolescent Psychiatry in the United States.” Psychiatric Times, Psychiatric Times, 1 Sept. 2003, www.psychiatrictimes.com/history-child-and-adolescent-psychiatry-united-states.
[2] – Breeding, John. “Electroshocking Children: Why It Should Be Stopped.” Mad In America, Science, Psychiatry, and Social Justice, 11 Feb. 2014, www.madinamerica.com/2014/02/electroshocking-children-stopped/.
[3] – Devitt, Michael. “Study: One in Six U.S. Children Has a Mental Illness.” AAFP Home, The American Academy of Family Physicians, 18 Mar. 2019, www.aafp.org/news/health-of-the-public/20190318childmentalillness.html.
Works Cited
– All of My Research Information Came From:
Breeding, John. “Electroshocking Children: Why It Should Be Stopped.” Mad In America, Science, Psychiatry, and Social Justice, 11 Feb. 2014, http://www.madinamerica.com/2014/02/electroshocking-children-stopped/.
Devitt, Michael. “Study: One in Six U.S. Children Has a Mental Illness.” AAFP Home, The American Academy of Family Physicians, 18 Mar. 2019, http://www.aafp.org/news/health-of-the-public/20190318childmentalillness.html.
Herman, Ellen. “Lauretta Bender, 1897-1987.” The Autism History Project, 2019, blogs.uoregon.edu/autismhistoryproject/people/lauretta-bender-1897-1987/.
Schowalter, John E. “A History of Child and Adolescent Psychiatry in the United States.” Psychiatric Times, Psychiatric Times, 1 Sept. 2003, http://www.psychiatrictimes.com/history-child-and-adolescent-psychiatry-united-states.
Wick, Jeannette Y. “Antipsychotics for Children With ADHD Should Be a Last Resort.” Pharmacy Times, Pharmacy & Healthcare Communications, 2 Feb. 2020, http://www.pharmacytimes.com/publications/issue/2020/February2020/antipsychotics-for-children-with-adhd-should-be-a-last-resort.
